AI Dental Clinic Automation: The 2026 Playbook to Fill More Chairs
Your clinic does not usually lose revenue because treatment quality is poor. It loses revenue in the gaps between patient intent and staff capacity. A missed call at 7:40 PM. A consultation lead that gets a callback the next day. A reminder sent once, then forgotten. A follow-up list that lives in a spreadsheet nobody checks after lunch.
Those gaps compound. If your clinic has 400 monthly appointments and a no-show rate of 12%, that is 48 empty slots. Even if only half of those could be recovered with better communication and scheduling, you gain 24 visits. At an average realized visit value of $140, that is $3,360 per month before hygiene plans, whitening upgrades, or long-term restorative work.
AI automation closes those gaps without creating chaos at the front desk. It routes inbound calls, confirms appointments with two-way replies, rebooks cancellations in minutes, and keeps treatment follow-up moving. You keep the human touch where it matters and automate the operational repetition where it does not.
This guide is built for clinic owners and managers who want practical execution. You will get workflow design, platform comparisons, numbers you can model, and a 30-day rollout path that works with existing systems. If you already use tools from our guides on CRM automation and WhatsApp business workflows, this post will connect them into one clinic growth engine.
The Revenue Leak Most Clinics Ignore
Dental growth rarely fails in marketing first. It fails in conversion operations. Front desks are overloaded with calls, insurance questions, rescheduling, reminders, and treatment follow-up. When volume spikes, consistency drops.
Research across primary care settings reports no-show variation from 5% to 55%. Dental clinics sit inside that operational reality: attendance depends on reminder timing, friction in rebooking, and response speed when patient intent is high. ADA Health Policy Institute reports also continue to track pressure on scheduling and staffing across practices. The result is predictable: even high-demand clinics leave revenue in open chair time.
If your clinic still treats reminders and follow-up as optional admin work, you are managing demand manually while competitors run demand as a system.
Three leak points appear in almost every practice:
- New enquiry response takes more than 10 minutes during peak hours.
- Reminders are one-way broadcasts instead of two-way confirmation flows.
- Pending treatment follow-up depends on memory, not workflow triggers.
Key Takeaway
AI automation in dental clinics is less about replacing people and more about preventing operational drop-offs that silently reduce bookings, attendance, and treatment acceptance.
Explore all industry-specific AI automation solutions we offer at Jogi AI.
What AI Dental Automation Actually Means
In a dental setting, AI automation is the coordination layer between patient communication, scheduling, and follow-up actions. It is not one chatbot. It is a set of connected flows that run with rules, context, and escalation.
Patient communication automation
AI drafts and sends reminders, confirmations, recall notices, and post-visit check-ins. Messages are personalized by appointment type, provider, and lead source. Replies like "Need to reschedule" trigger immediate alternate slot suggestions, not a manual callback queue.
Front-desk support automation
Voice and chat assistants handle routine queries: clinic hours, location, accepted insurance categories, preparation instructions, and first available slot windows. Complex clinical questions are flagged for staff and routed with context.
Treatment conversion automation
After consultation, the system sequences education, finance FAQ responses, and follow-up nudges at planned intervals. It can also log objections into your CRM and create tasks for treatment coordinators. This pairs well with the frameworks in AI lead generation funnels.
Operational intelligence
Automation does not just send messages. It monitors outcomes: confirmation rate, cancellation lead time, no-show risk, and reactivation lift. With this data loop, clinic managers optimize scripts and timing every week.
Evidence and Benchmarks That Matter
You do not need perfect data science to start. You need baseline metrics and realistic targets. Use this table as your benchmark grid for the first 90 days.
| Metric | Common Baseline | 90-Day Target | How AI Improves It |
|---|---|---|---|
| Missed call rate | 18% to 42% | Under 8% | After-hours AI answering plus overflow routing |
| No-show rate | 8% to 20% | 20% to 40% reduction | Two-way reminders, confirmations, and auto-rebook flows |
| Lead response speed | 15 to 180 minutes | Under 5 minutes | Instant AI qualification and booking link delivery |
| Treatment plan follow-up coverage | 40% to 65% | Above 90% | Automated multi-step communication sequences |
| Recall reactivation | 3% to 8% | 10% to 18% | Segmented recall campaigns with dynamic copy |
Why these targets? External healthcare studies consistently show that reminder systems and operational redesign reduce non-attendance in many settings, while response speed strongly influences conversion probability. Your exact results depend on list quality, staff handoff discipline, and system integration quality.
Six High-Impact Workflows to Deploy
1. Missed call capture and instant callback text
When your line is busy, AI sends a text within 20 seconds: "We missed your call. Want the earliest available hygiene or consultation slot?" The patient replies with one tap. The system proposes slots and books directly or queues a staff callback with context.
2. Two-way reminder and confirmation orchestration
Run three touches: 72 hours, 24 hours, and 3 hours before appointment. Patient replies "Confirm" or "Reschedule." Reschedule opens automated options. This mirrors what works in email automation systems but uses SMS/WhatsApp for faster response.
3. Cancellation rescue list auto-fill
When a slot opens, AI identifies patients on a priority list by treatment type, urgency, and location. It sends a first-wave offer and books the first confirmed response. Clinics with tight hygiene schedules can recover same-day revenue instead of leaving a chair idle.
4. Consultation lead qualification
AI asks standardized intake questions and captures preference data before your team calls: concern type, urgency, ideal appointment window, and budget constraints. This reduces unqualified appointments and improves case acceptance conversations.
5. Pending treatment follow-up sequence
After diagnosis, patients receive timed follow-up: education summary, finance options, social proof, and booking prompt. The workflow flags high-intent replies for immediate coordinator outreach. This is similar to support logic from AI customer support workflows, adapted for clinical operations.
6. Recall and reactivation campaigns
AI segments by last visit date, treatment history, and risk profile. It sends personalized recall nudges and tracks responses by segment. Over time, you learn which message framing performs best for each patient type.
Industry Use Cases by Clinic Type
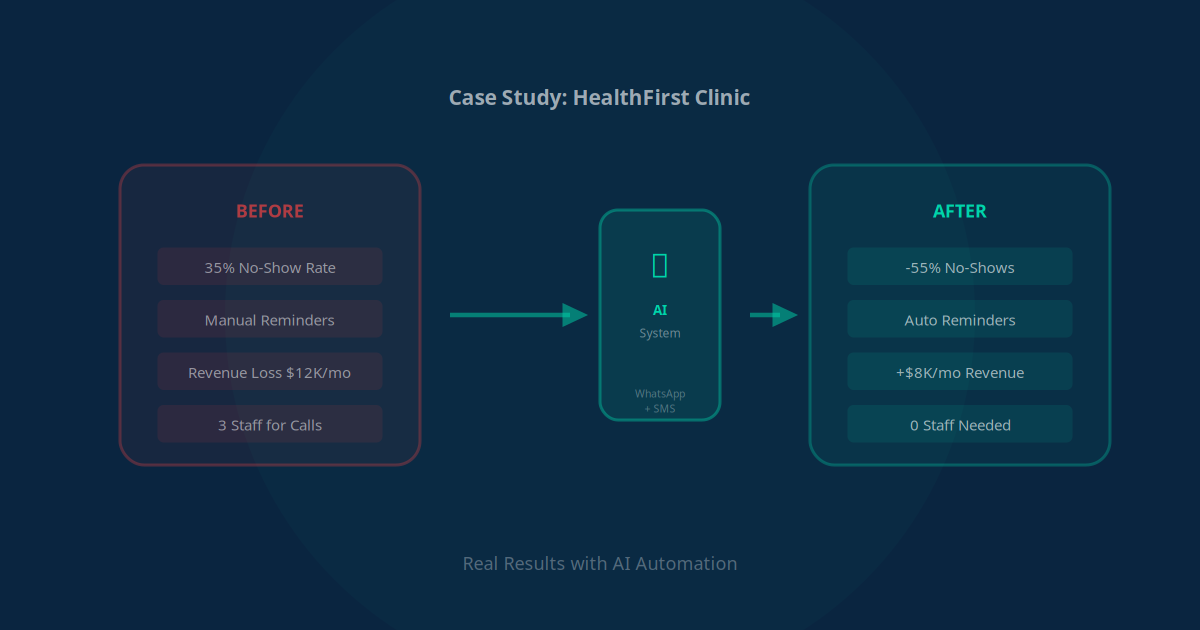
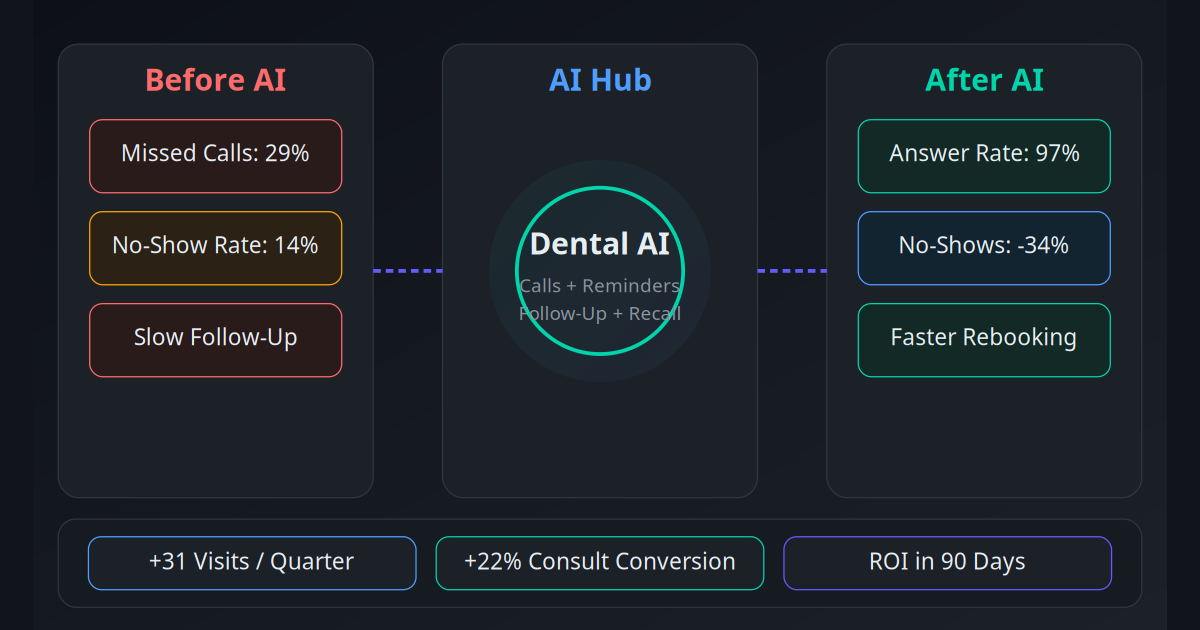
Single-Location Family Dental Clinic
Problem: Front desk missed 26% of lunchtime calls and no-shows averaged 14%. Solution: AI call capture + two-way reminder + cancellation rescue list. Result: no-shows dropped to 9% in 10 weeks and 31 extra appointments were recovered in one quarter.
Cosmetic Dentistry Practice
Problem: Consultation leads went cold because callbacks took 4 to 18 hours. Solution: instant lead qualification and same-minute booking links. Result: consultation-to-visit conversion rose from 34% to 52% and monthly whitening package sales increased 22%.
Orthodontic Clinic
Problem: High reschedule churn during school exam periods. Solution: AI reminder timing by age segment and proactive alternate slot suggestions. Result: appointment retention improved 19% and idle chair hours dropped by 11 hours per week.
Multi-Location Dental Group
Problem: inconsistent scripts and manual follow-up across branches. Solution: centralized automation templates with branch-level overrides and CRM dashboards. Result: follow-up coverage moved from 57% to 93% and standardization improved patient experience scores.
Implant-Focused Specialty Practice
Problem: high-value treatment plans stalled after first consult. Solution: staged educational follow-up with coordinator escalation signals. Result: accepted treatment value per month increased 17% after 90 days.
30-Day Implementation Roadmap
Execution speed matters more than tool perfection. Start narrow, validate fast, then expand. If you already run orchestration tools from Make vs Zapier vs n8n comparisons, the rollout is even faster.
Week 1, KPI baseline: Capture current missed call rate, no-show rate, response speed, and treatment follow-up coverage by provider and location.
Workflow mapping: Define exact triggers for missed calls, reminders, cancellations, and pending treatment stages. Assign clear ownership for exception handling.
System integration: Connect PMS/CRM, communication channels, and booking logic. Validate field mapping and avoid duplicate patient records.
Template and prompt design: Create compliant message templates, tone guidelines, and escalation scripts for clinical questions.
Pilot launch: Route 20% to 30% of eligible traffic for 7 days. Monitor failures daily, patch edge cases, and retrain front desk on handoff behavior.
Scale and optimize: Move to full traffic, review weekly KPIs, A/B test reminder timing, and tighten segments for recall and treatment conversion.
Governance: Add monthly QA for compliance, script drift, and integration health. Keep a human override path for every automation branch.
Tool and Platform Comparison
| Stack Option | Best For | Pros | Tradeoffs |
|---|---|---|---|
| PMS + Zapier + SMS + CRM | Fastest MVP | Quick launch, low setup friction | Can become brittle at scale |
| PMS + Make + WhatsApp + CRM | Branching workflows | Flexible logic and lower run cost | Requires better documentation |
| PMS + n8n self-hosted | Data control | High customization and privacy control | Needs technical ownership |
| Voice AI + CRM + calendar APIs | Call-heavy clinics | 24/7 coverage and instant booking | Conversation QA needed |
| Unified AI orchestration layer | Multi-location groups | Central governance with local routing | Higher initial design effort |
Many clinics evolve in stages: simple reminder automation first, then voice flows, then deeper orchestration with multi-agent logic. The architecture path is similar to what we explain in multi-agent AI systems for business and agentic AI operations.
ROI Math and Social Proof
"We stopped treating follow-up as admin overflow and started treating it as a production line. In 60 days, empty-chair days became rare."
— Operations Lead, 2-location dental clinicUse a conservative ROI model before rollout:
- Baseline: 320 monthly appointments, 12% no-show equals 38 no-shows.
- Automation impact: 30% no-show reduction recovers 11 appointments.
- Average realized value: 150 dollars per recovered appointment.
- Recovered monthly revenue: 1,650 dollars.
- Plus lead-speed lift: 8 extra consult bookings at 25% show and 40% acceptance can add 1,200 to 3,000 dollars.
- Total gross lift scenario: 2,850 to 4,650 dollars per month before labor savings.
When you layer in reduced manual reminder workload, fewer inbound schedule calls, and better recall consistency, most clinics hit break-even fast. A detailed custom projection can be generated with the same process used in our clinic no-show case study and voice AI deployment guide.
Mistakes That Kill Automation ROI
Automating before defining ownership
If nobody owns exception queues, automation creates silent backlog. Assign owners for every escalation path and response SLA.
Using generic templates for all patient segments
Recall patients, new consult leads, and high-value treatment follow-up need different tone and timing. One script for all reduces response quality.
Ignoring integration reliability
Broken field mapping can double-book slots or lose context. Monitor integration health daily in the first month.
Skipping compliance and consent controls
Operational automation must still respect communication consent, auditability, and protected data boundaries. Keep clinical guidance with licensed staff.
Chasing too many workflows in month one
Start with missed calls, reminders, and rebooking. Expand once KPI movement is proven. This stepwise discipline is the same principle behind reliable RAG system rollouts.
The Clinics Winning 2026 Will Run on Systems
Patient demand is not the bottleneck for most dental clinics. Operational consistency is. AI automation gives you consistent execution on calls, reminders, follow-up, and reactivation without burning out front-desk staff.
The best clinics will not be the ones with the fanciest tools. They will be the ones with clear workflows, strong data hygiene, and weekly KPI reviews. Start with one workflow, prove lift, and compound.
Competition in 2026 is moving from marketing spend to response speed and patient experience reliability. Clinics that automate responsibly will fill more chairs, protect team capacity, and convert more treatment plans.
Use the AI Business Twin for a free personalised analysis in under 10 minutes.
Frequently Asked Questions
What should a dental clinic automate first with AI?
Start with high-frequency and low-risk workflows: missed call capture, appointment reminders, confirmation tracking, and recall outreach. These workflows impact revenue in the first month and require less clinical risk than treatment recommendation automation. Once those are stable, add lead qualification and treatment follow-up.
How much can AI reduce dental no-shows?
Most clinics see meaningful reductions when they combine SMS plus WhatsApp reminders, two-way confirmation, and same-day fallback calls. A realistic benchmark is a 20% to 40% reduction in no-shows over 60 to 90 days, depending on baseline attendance, patient demographics, and reminder timing.
Is AI automation safe for patient communication and compliance?
Yes, when designed with role-based permissions, audit logs, approved templates, and protected data handling. Keep diagnostic and consent-sensitive communication routed to clinical staff, while AI handles operational messaging. Compliance improves when every reminder and follow-up is logged and standardized.
Do I need to replace my dental software to use AI automation?
No. Most clinics keep their existing PMS and CRM, then connect automation through APIs or workflow tools. The goal is orchestration, not replacement. You can start with one integration path, prove ROI, and expand without disrupting reception or clinical operations.
What ROI can a single-location dental clinic expect?
A common scenario is recovering 25 to 40 appointments per month from fewer no-shows and faster lead response. If average realized revenue per recovered visit is 80 dollars to 220 dollars, monthly gain can exceed 2,000 dollars to 8,000 dollars before treatment upsell effects. Many clinics recover implementation cost in one quarter.
How long does deployment take for a dental automation stack?
A focused rollout takes about 30 days. Week one maps workflows and KPIs. Week two connects systems and templates. Week three runs supervised pilot traffic. Week four scales to full traffic with weekly optimization. Complex multi-location governance can extend this to 45 to 60 days.